Introduction
Groin pain in basketball is rarely a simple, isolated injury. In high-performance settings, it more often reflects how an athlete is managing load across the hip-groin-pelvic complex during repeated on-court actions such as advancing the ball in transition, changing direction out of a crossover, closing out on a shooter, or creating separation with a v-cut.
These movements require repeated force absorption, redirection, and coordination between the trunk and lower extremity across multiple planes. While frameworks such as the Doha agreement help classify groin pain into clinical entities, basketball athletes often present with overlapping symptoms and compensatory movement strategies that extend beyond a single structure.
For medical and performance staffs, the objective is not only to identify the source of symptoms, but to understand how load is being distributed, how movement is adapting, and how to restore both tissue capacity and performance under basketball-specific demands.
What the Research Suggests
The current literature indicates that athletic groin pain is rarely confined to a single structure. The adductor longus, pubic aponeurosis, and rectus abdominis function as a shared load-bearing system across the anterior pelvis. In symptomatic athletes, pathology often involves multiple components of this system rather than an isolated tendon.
This is particularly relevant in basketball, where athletes are repeatedly exposed to lateral shuffling, opening up to sprint in transition, braking into a closeout, and planting to attack or recover defensively. These actions place consistent stress on the hip-groin complex through frontal and transverse plane loading.
Biomechanical studies show that athletes with groin pain often demonstrate altered movement strategies during change-of-direction tasks. This may include changes in trunk positioning, hip and knee mechanics, and ground reaction force profiles. On the court, this can present as difficulty planting and redirecting, inefficient breakdown into a closeout, or altered loading when attacking or recovering in space.
These movement adaptations may persist even after symptoms improve. Athletes may return to play feeling better, while still demonstrating differences in how they manage load compared to uninjured peers. This gap between symptom resolution and movement restoration is a key consideration in return-to-performance decisions.
Figure 1. Clinical Differentiation of Athletic Groin Pain in Basketball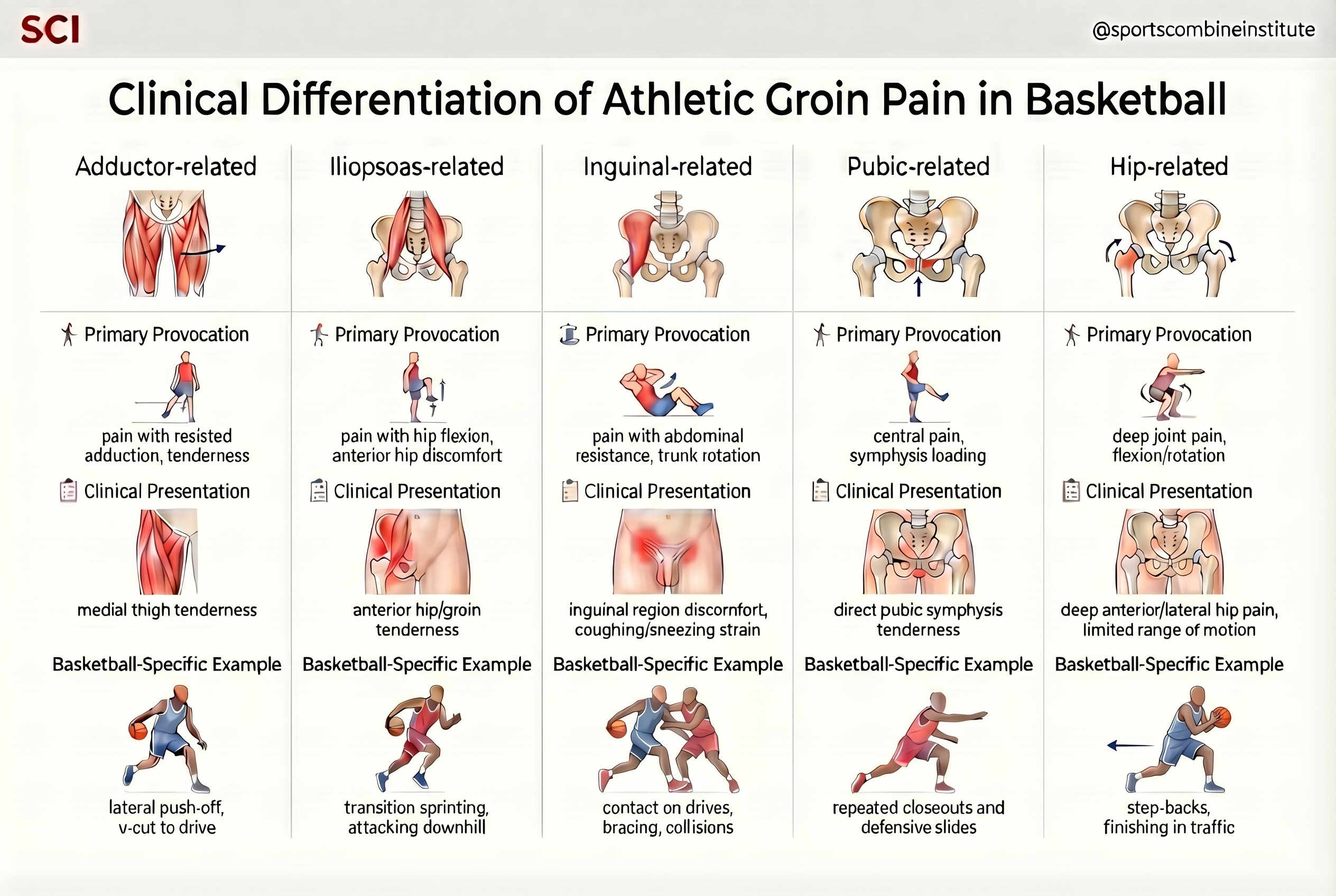
Clinical Differentiation
Effective management begins with identifying which structures are contributing to symptoms and how those structures respond to load. Differentiation should be guided by symptom provocation, palpation, and response to basketball-specific movement.
Adductor-Related Groin Pain
Adductor-related presentations are characterized by pain with resisted hip adduction, tenderness at the adductor origin or adductor complex, and symptoms that increase with frontal plane loading. In basketball, this may be provoked during lateral push-off, planting to change direction, or initiating a drive after a v-cut.
Iliopsoas-Related Groin Pain
Iliopsoas-related pain is commonly provoked with resisted hip flexion or hip flexor stretching. Athletes may report anterior hip or groin discomfort during repeated sprint efforts in transition or when aggressively driving the knee during acceleration.
Inguinal-Related Groin Pain
Inguinal-related presentations involve pain localized to the inguinal canal, often aggravated by abdominal resistance or increased intra-abdominal pressure. Symptoms may increase during trunk rotation, bracing, or absorbing contact when attacking or defending.
Pubic-Related Groin Pain
Pubic-related pain is typically localized over the pubic symphysis and may present as more central or bilateral discomfort. Symptoms often increase with repeated loading over time, such as multiple possessions of defensive slides, closeouts, or dense practice workloads.
Hip-Related Groin Pain
Hip-related presentations involve deeper joint symptoms and are often provoked by hip flexion, rotation, or compression. In basketball, this may be more apparent during step-backs, finishing in traffic, or other movements that require deep hip loading and rotational control.
Across all presentations, the key consideration is how load is provoking symptoms and how the athlete is responding to that load.
Figure 2. Load-Sharing Across the Hip-Groin Complex in Basketball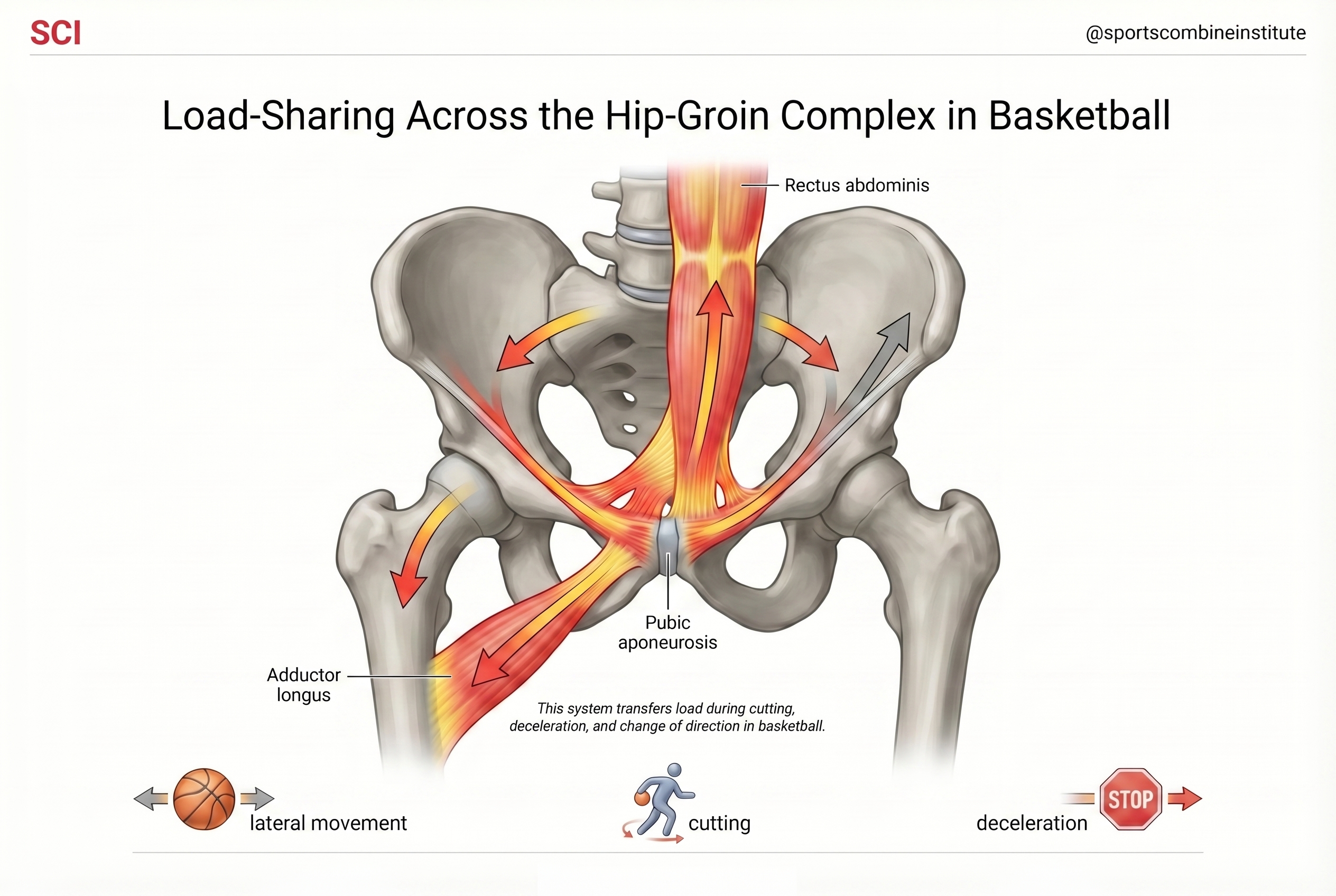
Implications for Medical and Performance Staffs
The management of groin pain should extend beyond the symptomatic structure and reflect the demands of basketball.
From a medical standpoint, restoring pain-free function in the involved tissue is necessary, but not sufficient. Athletes must also tolerate the forces required for multidirectional movement, including deceleration, lateral push-off, and rapid redirection.
From a performance standpoint, resilience in the hip-groin complex is built through progressive exposure to multidirectional loading. Basketball requires repeated braking into a closeout, redirecting off-ball movement, defending in lateral space, and creating separation through footwork under speed and fatigue.
From a return-to-performance standpoint, progression should be based on demonstrated capacity rather than time alone. Athletes should be able to tolerate basketball-specific tasks without symptom recurrence and without relying on compensatory movement strategies.
Practical Application
A structured progression from local tissue loading to full basketball performance integration is essential.
Early-stage management should focus on restoring tolerance within the symptomatic structure. This may include isometric loading for adductor-related pain, controlled hip flexor loading for iliopsoas-related presentations, or trunk-focused strategies for inguinal-related symptoms.
As symptoms improve, the focus should shift toward restoring force production across the hip-groin-pelvic system. Strengthening should include the adductors, hip flexors, and trunk musculature in ways that transfer to sport demands.
Movement integration is the next step. Planned basketball-specific patterns such as lateral slides, controlled deceleration into a closeout, redirecting out of a cut, and opening the hips in transition should be introduced and progressed.
On-court progression should reflect actual game demands, including reactive movement, repeated changes of direction, and tolerance to fatigue.
| Stage | Focus | Key Interventions | Basketball Application | Progression Criteria |
|---|---|---|---|---|
|
Stage 1 Symptom-Driven Loading |
Reduce irritability, restore tolerance | Isometrics, controlled loading based on presentation (adductor, hip flexor, or trunk-driven symptoms) | Limited on-court work, controlled positional drills | Pain controlled, tolerance to basic loading |
|
Stage 2 Force Development |
Build strength capacity across the hip-groin-pelvic complex | Progressive strengthening for adductors, hip flexors, trunk, and posterior chain | Linear movement, controlled acceleration and deceleration | Strength improving, minimal symptoms with loading |
|
Stage 3 Movement Integration |
Restore movement strategy and load absorption | Deceleration drills, planned change of direction, lateral movement, trunk control | Closeouts, lateral slides, planting and redirection | Tolerates multidirectional movement without compensation |
|
Stage 4 Basketball Performance |
Full sport-specific load tolerance | Reactive drills, high-speed change of direction, repeated efforts under fatigue | Game-speed cutting, defensive actions, transition play | Tolerates full practice and game demands |
Objective Testing and Strength Profiling
Objective strength assessment can provide additional context when managing groin pain in basketball, particularly when evaluating readiness for increased load and return to performance.
Isokinetic testing is commonly used to assess hip adduction and abduction strength, with attention to side-to-side asymmetries and adductor-to-abductor strength relationships. Deficits in adduction strength and imbalances across the hip have been associated with increased risk of groin pain in athletic populations.
However, these measures should not be interpreted in isolation. Strength symmetry in a controlled testing environment does not necessarily reflect how an athlete manages load during high-speed basketball actions such as cutting, decelerating, or reacting in space.
For this reason, strength testing is most useful when integrated with clinical findings and movement-based assessment. Improvements in isolated strength should translate to improved load tolerance during basketball-specific tasks.
| Measure | What It Tells You | Limitation |
|---|---|---|
| Adductor strength | Frontal plane force capacity | Does not reflect dynamic movement |
| Adductor:Abductor ratio | Hip strength balance | Does not capture coordination |
| Side-to-side asymmetry | Limb deficits | Not task-specific |
| Isokinetic peak torque | Isolated strength output | Limited transfer to sport |
Objective testing provides context, not conclusions. Strength symmetry in an isokinetic chair does not confirm readiness for game-speed cutting. Integrate testing data with clinical findings and observed movement quality during basketball-specific tasks.
Key Takeaways
- Groin pain in basketball reflects the interaction between tissue capacity and movement strategy rather than a single isolated injury.
- Clinical differentiation should be guided by symptom provocation and load response, not just anatomical location.
- Symptom resolution alone does not indicate readiness for return to performance.
- Effective management requires restoring both strength capacity and the ability to tolerate basketball-specific movement demands.
Summary
Athletic groin pain in basketball represents a complex interaction between structure, load, and movement. While classification frameworks help guide diagnosis, successful management depends on restoring the athlete’s ability to tolerate the demands of the sport.
In high-performance environments, the goal is not only to reduce pain but to re-establish a system capable of handling repeated, high-intensity, multidirectional movement. When both tissue capacity and movement strategy are addressed, return to performance becomes more complete.